P5) Stridor and fever in an infant
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a patient with stridor.
- Review the DDx considerations in stridor.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating patients with stridor.
History
Physical Exam
Labs
Provisional Diagnosis
Potential Acuity
What is your assessment of the likely acuity for this patient?
First Imaging Study
What is the first imaging study you will order?
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
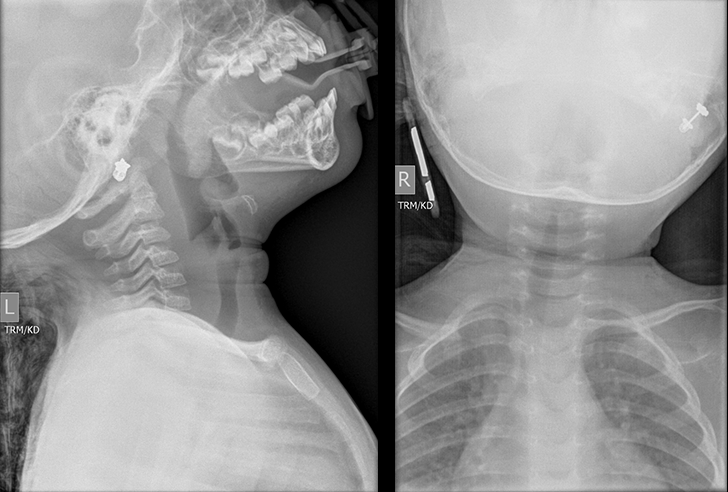
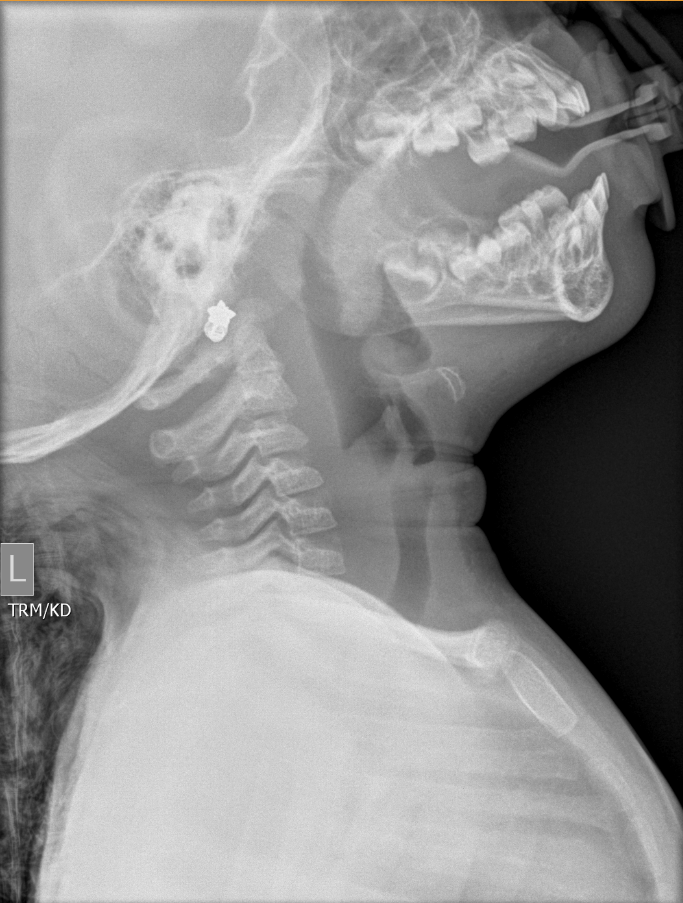
Soft-tissue lateral neck x-ray
The subglottic airway demonstrates pathological narrowing.
The size of the epiglottis is abnormally increased.

Watch our video
Second Imaging Study
What is the next imaging study you will order?
What is your Diagnosis now that you have seen the imaging results?
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
Assessment and Plan
Please provide your assessment and plan for this patient
Lessons Learned:
- Younger children (<5) are more likely to present with respiratory distress due to acute Epiglottitis.
- H. influenzae type b (Hib) is a common etiology of epiglottitis, particularly among unimmunized individuals.
- Epiglottitis can progress rapidly to life-threatening airway obstruction, thus airway management should be a primary focus of this presentation.
- While plain films of the neck are a diagnostic tool in the evaluation of epiglottitis, in the setting of acute respiratory distress they are not necessary as direct visualization during airway management is sufficiently diagnostic.
Socioeconomic Factors: There has been a decreased incidence in pediatric cases associated with H. influenzas infections (i.e., Epiglottitis) due to the launch of Hib vaccination programs in the US and other countries.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Contributors:
Jordan Turetsky, MS4 - Content Contributor
Khalida Clark - Content Contributor
Kevin Pierre, MD - Editor
Robbie Slater, MD - Supervising Editor
Bayar Batmunh, MS - Coordinator

{kind=link}
{kind=link}